Type 1 diabetes
Insulin dosing during a fast is dangerous without close clinical management. Hypoglycemia and diabetic ketoacidosis are real possibilities. Don't.

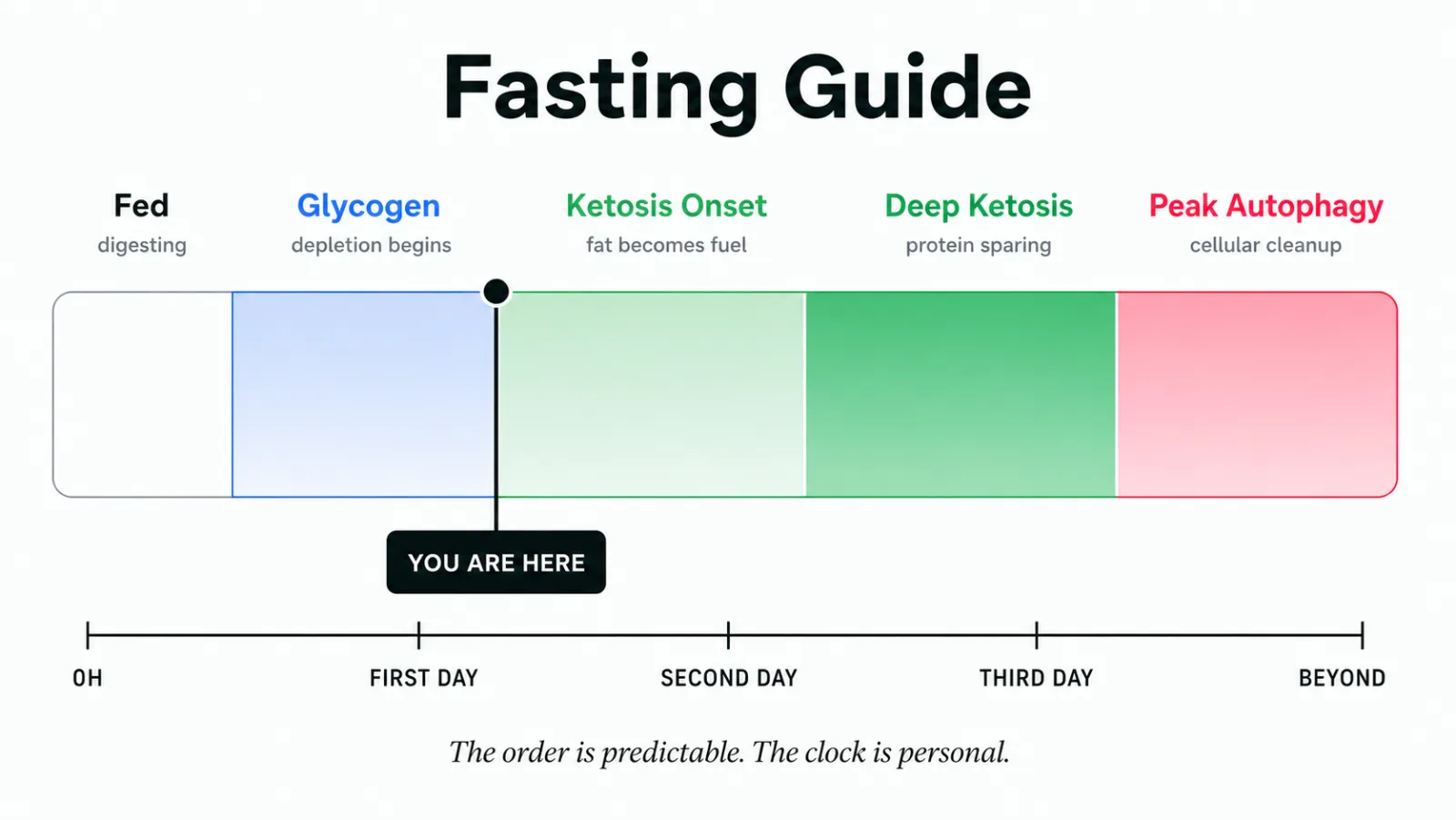
Fasting Guide · 5 stages explained
Fed, glycogen depletion, ketosis onset, deep ketosis, peak autophagy. The order is predictable. The clock is personal. This is what's actually happening - and who should not be doing it.
What an extended fast actually does, stage by stage. The order is consistent across people. The pace varies with activity level, glycogen stores, sleep, sex, and whether you've fasted before.
An extended fast isn't a longer skipped meal. It is a sequence of metabolic states your body moves through in a particular order - and most of what feels alarming during one of them is recognizable, expected biology.
The bad breath at the end of the first day. The chill on the second. The dizzy stand on the third. None of those are signs the fast is failing. Several of them are signs it's working as designed.
What follows is a grounded guide to the five stages: what's happening underneath, what's normal, what isn't, and - importantly - who should not be doing an extended fast at all.

This list is not a suggestion. Extended fasting interacts hard with several conditions, and the cost of getting it wrong is not theoretical.
Insulin dosing during a fast is dangerous without close clinical management. Hypoglycemia and diabetic ketoacidosis are real possibilities. Don't.
The energy demands of a developing or feeding child are not a place to apply caloric restriction experiments.
Anorexia, bulimia, binge-restrict cycles - fasting is often a familiar pattern wearing a wellness costume. If this is your history, this is not your tool.
Extended fasting is a physiological stressor. For people prone to post-exertional malaise, stacking that stressor on top of an already-fragile system can trigger a crash that takes weeks to recover from.
While some research is interesting on fasting and autoimmunity in remission, fasting during a flare is a different situation. Wait for a quiet window. Or skip it.
Insulin, sulfonylureas, several blood-pressure medications, thyroid medication timing. Don't fast through a med schedule without a clinician in the loop.
Also worth saying plainly: children, adolescents, and anyone underweight should not extended-fast. If you're new to fasting, start with 24 hours before you ever attempt 48 or 72. The data on side effects past the second day isn't subtle - most people experience them.
This is the baseline. Your last meal is still being broken down and absorbed. Insulin is elevated. Glucose from that meal is being shuttled into muscle and liver as glycogen, into fat cells as triglyceride, and into cells as immediate fuel.
Nothing about this state feels like fasting yet - and that's the point. The fast doesn't begin in the kitchen; it begins once digestion finishes its work. The shape of the meal you ate matters here: a high-carb dinner spikes insulin higher and delays the metabolic shift. A meal with more fat and protein tilts you toward a smoother transition.
If you intend to extended-fast, this is the last clean window to hydrate and salt your water - sodium reserves carry you further than you'd guess.

Insulin falls. Glucagon rises. Your liver begins releasing its glycogen stores back into circulation as glucose to keep your blood sugar stable. Muscle glycogen is broken down locally to power movement. The body is still running on sugar - but on sugar it stored, not sugar you ate.
This is the stage where hunger feels loudest. It comes in waves and passes. Mild headache, slight irritability, a vague restlessness - all expected. Most people meet this stage on the first day, late afternoon or evening, depending on when the last meal landed.
What helps: water with a real pinch of salt. A walk. A task that keeps your hands occupied. What doesn't help: standing in front of the pantry being curious about your willpower.
Glycogen runs low. Insulin reaches the floor. Without circulating glucose to default to, fat tissue begins releasing fatty acids, the liver converts them to ketone bodies - beta-hydroxybutyrate, acetoacetate, acetone - and your brain and muscles start burning them as fuel.
This is the switch. Hunger usually softens here, sometimes startlingly so. Mental clarity often arrives a few hours after the dip. The fruity or metallic taste in your mouth is acetone leaving on your breath - a small, real signal that the chemistry has changed.
It's also the stage where electrolytes start to matter. As insulin falls, your kidneys excrete more sodium. The dizziness on standing, the muscle twinge, the dull headache - these are usually sodium and magnesium losses, not the fast itself failing. Drink salted water. Add magnesium if you have it.


By the second day, ketone production has climbed and the body has settled into its alternate fuel system. The liver continues to generate a small amount of glucose from glycerol (released from fat) and from amino acids - gluconeogenesis - but the protein-sparing mechanisms have kicked in. Your body would rather burn fat than break down muscle, and most of the time it does.
Sleep often shifts here. Some people sleep less, lighter. Some report waking at small hours, awake and oddly clear. Cortisol is higher in this stage; your core temperature drops slightly; you'll likely feel colder than the room. None of those are wrong. They are the predictable physiological adjustments to running on a different fuel.
Hydration and electrolytes are not optional here. Two to three liters of salted water across the day, with potassium and magnesium if you can manage it. Coffee is fine; black tea is fine; bone broth is debated but is gentle and many people use it.
This is where the wellness internet gets loud and the human evidence gets quiet.
Autophagy is real - Yoshinori Ohsumi won the 2016 Nobel for the mechanistic work, and Valter Longo and Mark Mattson have published thoughtful clinical research on prolonged fasting and fasting-mimicking diets. What we can say with confidence: autophagy is a cellular recycling process that rises as insulin falls and ketones rise. It begins well before any 24-hour mark. It continues to increase across an extended fast.
What we cannot say honestly: that it peaks at exactly 48 hours, or 72, or any other clean number. Those specific timings come from rodent studies and cell-culture experiments. Direct measurement of autophagic flux in living humans is technically difficult and has not produced a clean curve. "Peak autophagy at 48 hours" is a wellness-marketing claim, not a published human finding.
What is reliable about the third day onward: appetite is usually quiet. Energy is variable - clear hours alternating with flat ones. Nausea and lightheadedness become common. Strong ketone breath. Sleep is often broken. This is when listening to your body matters most, and when severe symptoms are a reason to break the fast - not push through.

Free for core features. No card needed.
What's normal, what isn't, and the difference between an adaptation symptom and a stop sign.
Most people fasting past the second day experience some side effects - the published rate is roughly seven in ten. Recognizable adaptation is one thing. The list on the right is another.
| Normal - expected adaptation | Break the fast |
|---|---|
| Hunger waves that come and go | Severe dizziness that prevents normal activity |
| Fruity or metallic breath | Persistent nausea or any vomiting |
| Feeling cold | Heart palpitations or irregular heartbeat |
| Mild headache, mild fatigue | Confusion or trouble forming sentences |
| Dizziness when standing quickly | Severe, worsening headache |
| Lighter, broken sleep | Extreme weakness, can't safely move |
If your glucose drops below the low fifties and you feel unwell - not just a little flat, but actually unwell - that's also a stop sign. Break the fast with a small amount of fat or protein. Heavy carbs after an extended fast can cause a reactive glucose spike followed by a crash that feels worse than the symptom you were treating.
Your Apple Watch and your CGM already collect the signals that tell the real story. We translate them into plain language and surface the ones that matter.
A meaningful drop from your baseline past the second day is a real signal of physiological stress. We flag it gently - context, not alarm.
RHR elevated above your usual band often means dehydration. The fix is usually a glass of salted water, not breaking the fast.
A small drop in nighttime wrist temperature is one of the cleanest signals you've made the metabolic switch. We validate the chill.
If you wear a CGM, we read the glucose curve through the fast - the dawn rise, the slow descent into the sixties, the rapid drops worth noticing.
Fasting often compresses deep sleep and lightens the second half of the night. Knowing that's expected makes the morning less alarming.
One sentence per signal. Not a number. "Your wrist temperature dropped tonight - a normal sign of ketosis. Layer up."
Body Insights doesn't tell you to fast or not to fast. It reads what your wearable already records and translates whether what you're feeling matches the underlying data.
The first meal back is the part most people get wrong. A large, high-carb meal after two or three days of ketosis triggers a sharp insulin response, a reactive glucose drop, and often a small wave of feeling worse than you did fasting.
The gentler path: a small portion of fat and protein first. Bone broth. A few bites of avocado. A soft-cooked egg. Wait. Let your gut wake up. An hour or two later, add steamed vegetables, fermented foods, a small protein. Save anything starchy for the next real meal.
The longer the fast, the more gradual the refeed. Three days in deserves more than three minutes of patience getting out.
Five: fed, glycogen depletion, ketosis onset, deep ketosis, and peak autophagy. The order is consistent. The pace varies with activity, glycogen stores, sleep, sex, and fasting experience.
Type 1 diabetes, pregnancy, breastfeeding, eating disorder history, active ME/CFS or PEM-prone, active autoimmune flare, children and adolescents, anyone underweight, and anyone on insulin or sulfonylureas without clinical oversight.
Yes. Acetone - a ketone body - exits through the breath. The fruity or metallic taste is a real signal that fat-derived fuel has taken over.
We don't have a clean human answer. Most timing claims come from animal and cell studies. What we can say: autophagy rises across a fast as insulin falls and ketones climb. The exact peak in a human body has not been measured cleanly.
No. Sodium, potassium, and magnesium in water do not raise insulin in any meaningful way and become important past the first day. They prevent most of what people mistake for the fast going wrong.
No. Without a CGM, the glucose-curve layer drops out and HRV, RHR, wrist temperature, and sleep still carry the read. With one, you get a layer no other fasting app reads.
On-device. No account. No subscription required. No data sold. Ever.

Free for core features. Premium adds the deeper analytics layer.